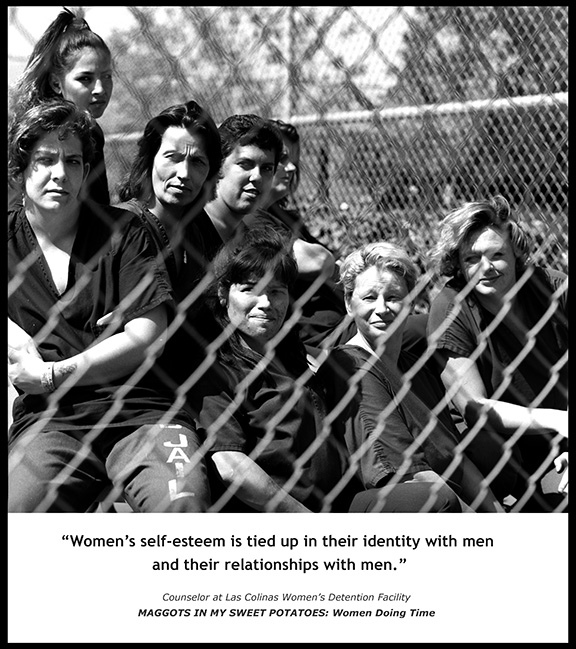
Photo by Susan Madden Lankford
“Housing First,” supported by the United States Department of Housing and Urban Development and nonprofit agencies throughout America, not only provides permanent homes for the homeless but also provides wraparound case management services to the tenants. This case management provides stability for homeless individuals, which increases their success. It allows for accountability and promotes self-sufficiency.
The housing provided through government-supported Housing First programs is permanent and “affordable,” meaning that tenants pay 30% of their income towards rent. Housing First initially targeted individuals with disabilities. This housing is supported through two HUD programs: the Supportive Housing Program and the Shelter Plus Care Program. The Housing First model has been recognized by the Substance Abuse and Mental Health Services Administration as an Evidence-based practice.
Principles of Housing First are: 1) Move people into housing directly from streets and shelters without preconditions of treatment acceptance or compliance; 2) The provider is obligated to bring robust support services to the housing. These services are predicated on assertive engagement, not coercion; 3) Continued tenancy is not dependent on participation in services; 4) Units targeted to most disabled and vulnerable homeless members of the community; 5) Embraces harm-reduction approach to addictions rather than mandating abstinence. At the same time, the provider must be prepared to support resident commitment to recovery; 6) Residents must have leases and tenant protections under the law; 7) Can be implemented as either a project-based or scattered-site model.[6]
Housing First is currently endorsed by the United States Interagency Council on Homelessness as a “best practice” for governments and service-agencies to use in their fight to end chronic homelessness in America.
Housing First programs currently operate throughout the United States in cities such as New Orleans, LA; Plattsburgh, NY; Anchorage, AK; Minneapolis, MN; New York City; District of Columbia; Denver, CO; San Francisco, CA; Atlanta, GA; Chicago, IL; Quincy, MA; Philadelphia, PA; Salt Lake City, UT; Seattle, WA; Los Angeles; Austin, TX and Cleveland, OH, among many others, and are intended to be crucial aspects of communities’ so-called 10-Year Plans To End Chronic Homelessness.
On June 11, 2014 the “100,000 Homes Campaign” in the United States, launched in 2010 to “help communities around the country place 100,000 chronically homeless people into permanent supportive housing,” announced that it reached its four-year goal of housing 100,000 homeless people nearly two months before its July 29 deadline.
Here are some “Housing First” results:
In Massachusetts, the Home & Healthy for Good program reported some significant outcomes that were favorable especially in the area of cost savings.
The Denver Housing First Collaborative, operated by the Colorado Coalition for the Homeless, provides housing through a Housing First approach to more than 200 chronically homeless individuals. A 2006 cost study documented a significant reduction in the use and cost of emergency services by program participants as well as increased health status. Emergency room visits and costs were reduced by an average of 34.3% . Hospital inpatient costs were reduced by 66%. Detox visits were reduced by 82%. Incarceration days and costs were reduced by 76%, and 77% of those entering the program continued to be housed in the program after two years.
Researchers in Seattle, partnering with the Downtown Emergency Service Center, found that providing housing and support services for homeless alcoholics costs taxpayers less than leaving them on the street, where taxpayer money goes towards police and emergency health care. Results of the study funded by the Substance Abuse Policy Research Program of the Robert Wood Johnson Foundation appeared in the Journal of the American Medical Association April, 2009. This first US controlled assessment of the effectiveness of Housing First specifically targeting chronically homeless alcoholics showed that the program saved taxpayers more than $4 million over the first year of operation. During the first six months, even after considering the cost of administering the housing, 95 residents in a Housing First program in downtown Seattle, the study reported an average cost-savings of 53%—nearly US $2,500 per month per person in health and social services, compared to the per month costs of a wait-list control group of 39 homeless people. Further, stable housing also results in reduced drinking among homeless alcoholics.
In Utah, there has been a 72% homelessness decrease overall since enacting the plan in 2005, according to the Utah Division of Housing and Community Development.
In August 2007, HUD reported that the number of chronically homeless individuals living on the streets or in shelters dropped by an unprecedented 30%, from 175,914 people in 2005 to 123,833 in 2007. This was credited in part to the “housing first” approach; Congress in 1999 directed that HUD spend 30% of its funding on the method.
In September 2010, it was reported that the Housing First Initiative had significantly reduced the chronic homeless single person population in Boston, although homeless families were still increasing in number. Some shelters were reducing the number of beds due to lowered numbers of homeless, and some emergency shelter facilities were closing, especially the emergency Boston Night Center. By 2015, Boston Mayor Marty Walsh had announced a 3-year plan to end chronic homelessness, focusing on coordinating efforts among public agencies and nonprofit organizations providing services to homeless men and women.
In South Australia, the State Government of Premier Mike Rann (2002 to 2011) committed substantial funding to a series of initiatives designed to combat homelessness. The Rann Government established Common Ground Adelaide, building high-quality inner city apartments (combined with intensive support) for “rough sleeping” homeless people. The government also funded the Street-to-Home program and a hospital liaison service designed to assist homeless people who are admitted to the emergency departments of Adelaide’s major public hospitals. Rather than being released back into homelessness, patients identified as rough sleepers are found accommodation backed by professional support. Common Ground and Street-to-Home now operate across Australia in other states.
In its Economic Action Plan 2013, the Federal Government of Canada proposed $119 million annually from March 2014 until March 2019—with $600 million in new funding—to renew its Homelessness Partnering Strategy (HPS). In dealing with homelessness in Canada, the focus is on the Housing First model. Thus, private or public organizations across Canada are eligible to receive HPS subsidies to implement Housing First programs. In 2008, the Federal Government of Canada funded a five-year demonstration program, the At Home/Chez Soi project, aimed at providing evidence about what services and systems best help people experiencing serious mental illness and homelessness. Launched in November 2009 and ending in March 2013, the At Home/Chez Soi project was actively addressing the housing need by offering Housing First programs to people with mental illness who were experiencing homelessness in Vancouver, Winnipeg, Toronto, Montréal and Moncton. In total, At Home/Chez Soi has provided more than 1,000 Canadians with housing.
Housing First has grown in popularity in Canada and used in many Canadian ten-year plans to end homelessness, such as those in Edmonton and Calgary. Housing First: A Canadian Perspective is spearheaded by Pathways to Housing Calgary and director Sue Fortune. Canadian adaptations to Housing First have demonstrated positive outcomes as documented on the website: www.thealex.ca (Housing Programs; Pathways to Housing). Canadian implementations of Housing First must be tailored to Canadian homelessness, resources, politics and philosophy.
In Calgary, Alberta, the Alex Pathways to Housing Calgary which opened in 2007, had 150 individuals in scatter-site homes in 2013. Clients pay 30% of their income towards their rent: 85 percent of Pathways to Housing clients receive Assured Income for the Severely Handicapped benefits and 15% receive Alberta Works. The Alex Pathways to Housing uses a Housing First model, but it also uses Assertive Community Treatment (ACT), an integrated approach to healthcare where clients access a team of “nurses, mental health specialists, justice specialists and substance abuse specialists.”
Director Sue Fortune is committed to the 10 Year Plan To End Homelessless in the Calgary Region. Fortune reported that the Housing First approach resulted in a 66% decline in days hospitalized (from one year prior to intake compared to one year in the program), a 38% decline in times in emergency room, a 41% decline in EMS events, a 79% decline in days in jail and a 30% decline in police interactions.She reported that fewer than 1% of existing clients return to shelters or rough sleeping; clients spend 76% fewer days in jail and clients have a 35% decline in police interactions.
In 2007 the centre-right government of Matti Vanhanen began a special program of four wise men to eliminate homelessness in Finland by 2015. The program to reduce long-term homelessness targets hard-core homeless people,assessed on the basis of social, health and financial circumstances. The program to reduce long-term homelessness focuses on the 10 biggest urban growth centers, where also most of the homeless are to be found. The main priority, however, is the Helsinki Metropolitan Area, and especially Helsinki itself, where long-term homelessness is concentrated.
The program is structured around the housing first principle. Solutions to social and health problems cannot be a condition for organising accommodation: on the contrary, accommodation is a requirement which also allows other problems of people who have been homeless to be solved. Having somewhere to live makes it possible to strengthen life management skills and is conducive to purposeful activity.
Because of all the reasons there are for long-term homelessness, if it is to be cut there need to be simultaneous measures at different levels, i.e. universal housing and social policy measures, the prevention of homelessness and targeted action to reduce long-term homelessness.
The program’s objectives are to eliminate homelessness entirely by 2015 and to take more effective measures to prevent homelessness.
In France the government launched a Housing First-like program in 2010 in 4 majors cities: Toulouse, Marseille, Lille and Paris called “Un chez-Soi d’abord”. It follows the same principles as the Canadian and US programs, focusing on the homeless people with mental illness or addicted to drugs or alcohol. The plan is on a 3-year basis for each individual, sheltered in an apartment lent by a non-government organization. Several NGOs are involved in this experiment, they are assuring the rental management as well as the social support for the housed people.
Those NGOs are linked with scientists investigating the results of the experiment and serve as a relay for informations and status reports on the targeted public. The lead team of “Un chez-soi d’abord” is expecting results to be published around 2017.